ICMS Billing Rate Designations and Multifactorial Analysis
HSH’s ICMS program operates within a capped budget. Billing rate designations are applied through a consistent, data-driven distribution of limited resources across slots with varying levels of case management need. This guide explains how designations work, what drives them, and how case managers can support accurate billing.

ICMS Billing Rates
ICMS includes four billing rates across two service intensity tiers (low and high), based on household type and expected level of service. Each billing rate is associated with a corresponding caseload weight, which indicates how many slots of that type make up a full caseload for a case manager. Caseloads may include slots with varying billing rates, but total caseload weight must not exceed 100% of a full caseload (1.0 FTE) for each case manager.
Use the ICMS Snapshot to monitor caseload weights and distributions.
Low Service Intensity Tier
Single Adult
$258.75/month
Caseload Weight: 1:40
Family
$345/month
Caseload Weight: 1:30
Minimum Requirements/Month: 1 In-Person Encounter | 2 Services
High Service Intensity Tier
Single Adult
$517.50/month
Caseload Weight: 1:20
Family
$690/month
Caseload Weight: 1:15
Minimum Requirements/Month: 2 In-Person Encounters | 2 Services
Family Billing Rate Requirements
To qualify for the family billing rate, all of the following must be true:
- Household includes at least one dependent
- Household composition is accurate in CHAMP
- Record is confirmed within the past year
Billing rates are reviewed monthly and adjusted based on program-wide designation logic. Because the number of high-tier designations are limited by budget caps, increasing one slot from low to high requires a corresponding decrease elsewhere in the program, which may occur inside or outside of a provider’s own caseload.
Billing Rate Designation Logic
Each ICMS slot is evaluated each month through a structured logic flow to determine whether it is auto-retained at a high or low rate, or whether it enters the multifactorial analysis pool. The flow chart below illustrates how each slot is designated.
Billing Rate Designation Logic Flow
Auto-Retained High/Low: Automatic billing rate designation based on clearly defined criteria.
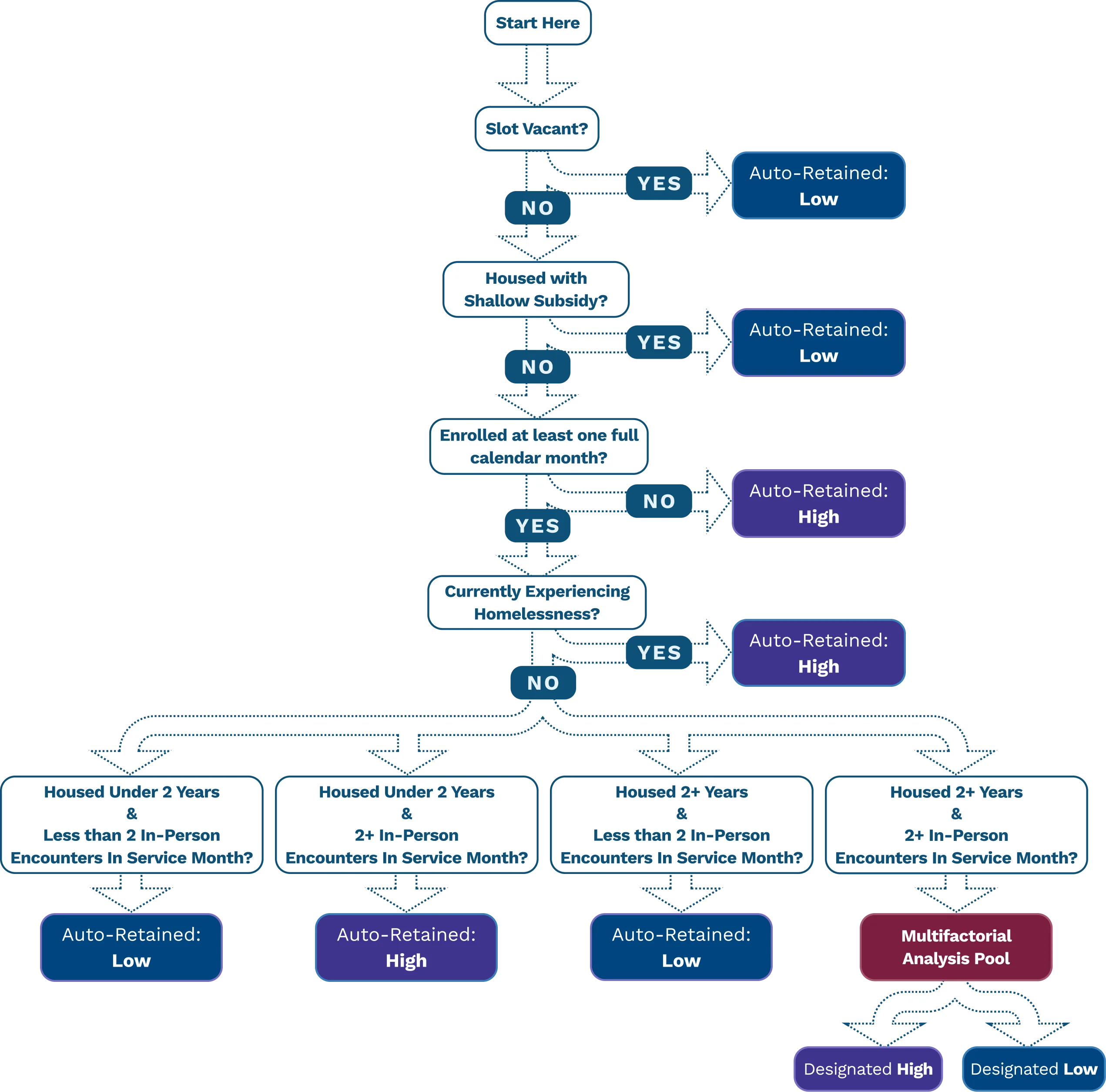
The Three Designation Pathways
Pathway 1
Auto-Retained: High
A slot is automatically designated at the high rate when any of the following apply:
- Participant has been checked in to the ICMS slot less than one full calendar month
- Participant is currently experiencing homelessness
- Participant is housed under 2 years AND had 2 or more in-person encounters in the service month
Pathway 2
Auto-Retained: Low
A slot is automatically designated at the low rate when any of the following apply:
- Slot is vacant
- Participant is housed with a shallow subsidy
- Participant is housed under 2 years AND had fewer than 2 in-person encounters in the service month
- Participant is housed 2 or more years AND had fewer than 2 in-person encounters in the service month
Pathway 3
Multifactorial Analysis Pool
A slot enters the multifactorial analysis pool when:
- Participant is housed 2 or more years AND had 2 or more in-person encounters in the service month
After auto-retaining eligible slots at high or low rates, remaining slots enter the multifactorial analysis pool, where available high-rate designations are assigned based on prioritization; all other slots are assigned the low rate.
Tip: Use the ICMS Snapshot to monitor caseload weights and distributions. The ICMS Snapshot is a daily report that provides a comprehensive view of case-level information and key indicators used to monitor billing rates and service delivery.
Multifactorial Analysis
The multifactorial analysis is a structured, automated review of factors across multiple case dimensions — participant need, service delivery, documentation, and outcomes — considered together to help prioritize high billing rate designations within program budget caps. The relative importance of factors may vary month to month based on available program data and budget.
All slots that make it into the multifactorial analysis pool compete for a finite number of high billing rate designations available. Not all slots with high needs or service intensity will be designated with a high billing rate in a given month.
Key Dimensions and Example Factors
*The factors listed below represent an example portion of relevant factors only.
Acuity and Case Management Needs
Example factors: Assessment content • Recent hospitalization • Complex health condition
Service Intensity
Example factors: In-person encounters • Number of services provided • Care Plan / needs alignment
Documentation Completeness and Quality
Example factors: Timely assessment completion • Care Plan updates • Required consents
Outcomes
Example factors: Housing retention • Increased income • Reduced crisis system utilization
Program Budget Cap
Number of high billing rate designations available in a given month
The multifactorial analysis is distinct from disallowed cost reviews, however, it can be possible that the factors leading to disallowed costs also lead to lower prioritization for a high billing rate in the multifactorial analysis pool.
Common Considerations for Billing Rate Designations
No single factor determines the rate in the multifactorial analysis pool. It is always based on a combination of factors and available program information — not one data point alone.
Higher acuity and service intensity increase prioritization for the high billing rate in the multifactorial analysis — but do not guarantee it, given the program-wide cap on high-rate designations.
In-person encounters outweigh unsuccessful outreach when service intensity is evaluated in the multifactorial analysis.
Strong, complete documentation in CHAMP ensures participant needs and services are correctly reflected — and directly supports billing rate designation.
Billing rate designations are reviewed monthly and may be adjusted based on updated information.
Billing rate designations are not arbitrary and not punitive.
Designations are applied prospectively — not retroactively.
The key case dimensions used in the multifactorial analysis can be monitored in the ICMS Snapshot.
CHAMP and Funding
“If your work is not documented in CHAMP, it cannot be used to support billing.”
HSH relies on CHAMP documentation to:
- Understand participant needs and acuity to coordinate appropriate care
- Support accurate Medi-Cal claims and program billing
- Evaluate and report on the performance of LA County’s homelessness response system over time, which impacts overall program funding and sustainability
Documentation quality and completeness directly impacts how participant case management needs and service intensity are reflected in the billing rate review.
Monthly Billing Rate Review Cycle
Service month closes (documentation deadline)
Automated program-wide review and designations
Adjustments applied by HSH and reflected in following service month invoice
Where to View Billing Rate Designations
The ICMS Program Summary Report (PSR) shows:
- Which slots will retain their current billing rate
- Which slots are flagged for adjustment
- Which slots are vacant
- Each slot’s projected billing rate for the next invoice
- Trends for the fiscal year
ICMS billing rate designations and adjustments are standardized program-wide and applied consistently across all providers and slots. However, not all providers will have an equal proportion of slots designated with a high billing rate.